Drug prices by country
Sources and derivations for Figure 2 of One Drug, Many Prices: A Proposal to Reform US Healthcare Pricing. Back to overview.
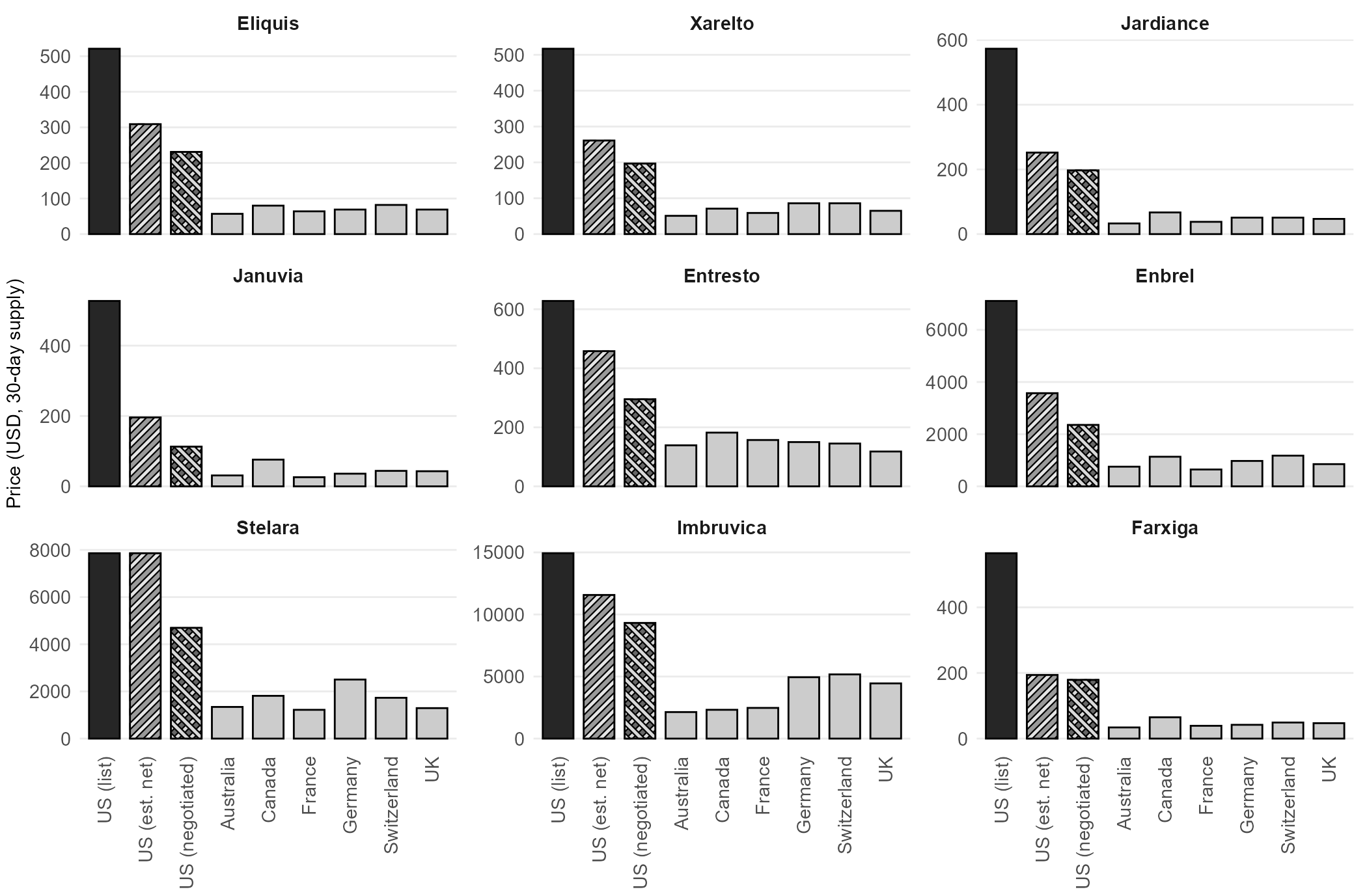
Nine widely used medications, all selected for Medicare negotiation under the Inflation Reduction Act, cost substantially less in peer developed countries than in the United States. The comparison covers US list prices, estimated US net prices (after rebates and discounts), Medicare's new IRA-negotiated prices, and prices in six peer countries. This page documents every figure shown in Figure 2.
How to read the sources
For each drug, the nine bars represent:
- US (list): the US wholesale acquisition cost (WAC), which is what uninsured patients face at retail pharmacy.
- US (est. net): the estimated US net price paid by private insurers after manufacturer rebates and discounts, derived from SSR Health data and SEC filings as reported in Wouters et al. (JAMA 2025).
- US (negotiated): the Medicare Maximum Fair Price negotiated under the Inflation Reduction Act, effective 2026.
- Australia, Canada, France, Germany, Switzerland, UK: the official reimbursed price in each country, as compiled in the same Wouters et al. dataset.
All prices are denominated in US dollars per 30-day supply at the adult maintenance dose used by Wouters et al. Expand any drug below to view the exact figures.
Notes on scope
- The nine drugs are the first ten drugs selected by CMS for Medicare negotiation based on Medicare Part D spending, minus insulin aspart. Insulin aspart is excluded because international prices are reported per unit rather than per 30-day supply, making a direct comparison imprecise.
- Every other country shown negotiates drug prices through centralized purchasing (a single government or government-authorized body bargaining on behalf of all covered patients). The United States, until the Inflation Reduction Act of 2022, did not.
- The US net price is an estimate because exact rebates are confidential. It is the best publicly available figure, derived from manufacturer SEC filings and SSR Health's gross-to-net model.
- The Medicare negotiated prices take effect in 2026 and were announced by CMS in August 2024.
Per-drug figures
Eliquis (apixaban), 30-day supplyIRA Year 1
- US (list)
- $521
- US (est. net)
- $309
- US (negotiated)
- $231
- Australia
- $57
- Canada
- $80
- France
- $64
- Germany
- $69
- Switzerland
- $82
- UK
- $69
Xarelto (rivaroxaban), 30-day supplyIRA Year 1
- US (list)
- $517
- US (est. net)
- $261
- US (negotiated)
- $197
- Australia
- $51
- Canada
- $71
- France
- $59
- Germany
- $86
- Switzerland
- $86
- UK
- $65
Sources: Wouters et al. JAMA 2025; CMS MFP.
Jardiance (empagliflozin), 30-day supplyIRA Year 1
- US (list)
- $573
- US (est. net)
- $252
- US (negotiated)
- $197
- Australia
- $33
- Canada
- $67
- France
- $38
- Germany
- $51
- Switzerland
- $51
- UK
- $47
Sources: Wouters et al. JAMA 2025; CMS MFP.
Januvia (sitagliptin), 30-day supplyIRA Year 1
- US (list)
- $527
- US (est. net)
- $196
- US (negotiated)
- $113
- Australia
- $31
- Canada
- $76
- France
- $26
- Germany
- $36
- Switzerland
- $44
- UK
- $43
Sources: Wouters et al. JAMA 2025; CMS MFP.
Entresto (sacubitril/valsartan), 30-day supplyIRA Year 1
- US (list)
- $628
- US (est. net)
- $458
- US (negotiated)
- $295
- Australia
- $139
- Canada
- $182
- France
- $157
- Germany
- $150
- Switzerland
- $145
- UK
- $118
Sources: Wouters et al. JAMA 2025; CMS MFP.
Enbrel (etanercept), 30-day supplyIRA Year 1
- US (list)
- $7,106
- US (est. net)
- $3,572
- US (negotiated)
- $2,355
- Australia
- $754
- Canada
- $1,135
- France
- $646
- Germany
- $974
- Switzerland
- $1,177
- UK
- $852
Sources: Wouters et al. JAMA 2025; CMS MFP.
Stelara (ustekinumab), 30-day equivalentIRA Year 1
- US (list)
- $13,836
- US (est. net)
- $7,860
- US (negotiated)
- $4,695
- Australia
- $1,342
- Canada
- $1,813
- France
- $1,220
- Germany
- $2,504
- Switzerland
- $1,730
- UK
- $1,292
Sources: Wouters et al. JAMA 2025; CMS MFP.
Imbruvica (ibrutinib), 30-day supplyIRA Year 1
- US (list)
- $14,934
- US (est. net)
- $11,571
- US (negotiated)
- $9,319
- Australia
- $2,137
- Canada
- $2,320
- France
- $2,472
- Germany
- $4,944
- Switzerland
- $5,172
- UK
- $4,447
Sources: Wouters et al. JAMA 2025; CMS MFP.
Farxiga (dapagliflozin), 30-day supplyIRA Year 1
- US (list)
- $565
- US (est. net)
- $194
- US (negotiated)
- $179
- Australia
- $34
- Canada
- $65
- France
- $39
- Germany
- $42
- Switzerland
- $49
- UK
- $47
Sources: Wouters et al. JAMA 2025; CMS MFP.
Notes on method
- Wouters et al. (JAMA 2025) is the single primary source for the list, net, and peer-country prices. The paper collected drug prices in the US and six other developed nations (Australia, Canada, France, Germany, Switzerland, UK) for the drugs selected in the first round of Medicare negotiation under the Inflation Reduction Act. Peer-country prices are the official reimbursed prices in each country (ex-factory or equivalent), converted to USD at the exchange rates used in the paper.
- Net US prices are estimates because exact rebates remain confidential. The figures use SSR Health's gross-to-net model, which draws on manufacturer SEC filings (10-K and 10-Q) and is the most widely cited such model in health economics.
- Medicare negotiated prices come directly from CMS's published fact sheet on the first ten drugs selected under the Medicare Drug Price Negotiation Program. They take effect in 2026.
- Exchange rates and time points follow Wouters et al. 2025. Peer-country prices can shift modestly with exchange rates, but the ratios shown here are stable across common reference periods.